
▼This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Please report any adverse events via your national reporting system. Adverse events can also be reported to Alexion Pharmaceuticals by contacting: https://contactazmedical.astrazeneca.com.
Please refer to the Summary of Product Characteristics for further information.
healthcare professional
- RGI-C scores improved from baseline to Week 24 and from baseline to Week 48, with 90% (9/10) patients (95% CI: 55–100%) and 89% (8/9) patients (95% CI: 52–100%), respectively, meeting the response criteria†9
- The median RGI-C score was increased by 2.0 points at Week 24 and by 2.3 points at Week 48 (P = 0.004), demonstrating a substantial and continued healing of rickets9
- Median RGI-C scores reflected improvements in mineralization as early as month 3, which were generally maintained over 7 years of treatment as Median RGI-C scores showed significant improvements compared to baseline at most time points (p<0.05)2
- At year 1, 89% (8 out of 9) of evaluable patients had RGI-C scores of +2 (responders) or higher, and by year 7, all evaluable patients (7 out of 7) had reached this level2
Patients from Study 1 show substantial and continued healing based on the RGI-C scale9
†Wilcoxon signed-rank tests.
- At Month 6 of treatment with STRENSIQ®, a significant improvement in RGI-C score was observed; P < 0.0001 (n = 69)5
- 58% (40/69) of patients were considered responders, with 9% (6/69) of patients achieving a score of +3, indicating complete or near-complete healing of HPP-related skeletal manifestations5
- Results at Year 1 of treatment were consistent with Month 6; P < 0.0001 (n = 69)5
- 72% (50/69) patients were considered responders at Year 1, with four patients achieving a score of +35
-
After 6 weeks of treatment with STRENSIQ®, the median RGI-C score had improved significantly (+1.0 [0.0, +2.0; min, max ]; P = 0.001), and further improvements occurred by 6 months and persisted through to 5 years (+2.2 [+1.7, +2.7 ]; P = 0.0005)6
- By contrast, no significant change occurred in the RGI-C score of the historical controls spanning up to 2 years6
- The RGI-C responder analysis showed 69% (9/13) of the treated patients achieved an RGI-C score of at least +2 at 6 months of therapy (LOCF data imputation applied) compared with 6% (1/16) of the historical control (P = 0.007)6
- After 2 years, 75% of treated patients considered responders experienced substantial or near/complete healing of HPP-related rickets, as measured by the RGI-C scale, which steadily improved to 92% at 5 years6
Long-term treatment with STRENSIQ® may help to improve bone mineralisation in patients with HPP.6
*An open-label, Phase 2 study evaluating the safety, tolerability, and efficacy of treatment with STRENSIQ® for up to 5 years; 13 patients were enrolled, aged 6- to 12-years-old at baseline, with either infantile- or childhood-onset HPP.6
Plasma PLP: one of the natural substrates of TNSALP and the principal circulating form of vitamin B6, which can act as a supplementary diagnostic tool when looking at laboratory parameters for HPP.6,8,9
One of the co-primary endpoints of this study, change in PPi at 6 months, did not reach statistical significance when comparing the control group to the treatment group.6- Of the 11 patients who required respiratory support at baseline (including mechanical ventilation, CPAP, or supplemental oxygen), 9/9 patients (100%) no longer required support by the study's end.2
- In patients who initially required ventilation, the ability to wean from ventilatory support following STRENSIQ® treatment was associated with, and preceded by, better skeletal mineralisation as documented by the RGI-C scores.2
*An open-label, single arm, Phase 2 study evaluating the safety, tolerability, and efficacy of treatment with STRENSIQ® for up to 7 years in 11 patients with perinatal and infantile HPP occurring before 6 months of age, ranging in age at baseline from 2 weeks to 3 years.2,9
- Of the 69 patients in the study, 45 (65%) did not require respiratory support at baseline, and 38 (84%) remained ventilator-free throughout the study.5
- The Kaplan-Meier estimate of the ventilator-free survival rate at Year 6 for patients who did not require respiratory support at baseline was 84%, and the overall survival rate at Year 6 for all patients was 80%.5
-
Growth improvements were observed, with significant increases in both length/height and weight z-scores from baseline to the last assessment
(P = 0.0025 and P = 0.0001, respectively).5 - Skeletal mineralisation, as measured by ALP activity, showed continued improvement throughout treatment.5
*An open-label, Phase 2 study evaluating study evaluating the safety, tolerability, and efficacy of treatment with STRENSIQ® for up to 6 years; 69 patients were enrolled, aged ≤5 years at baseline, with HPP and sign/symptom onset before age 6 months.5
- STRENSIQ® promotes significant catch-up growth in paediatric patients with HPP6
{kind=link}
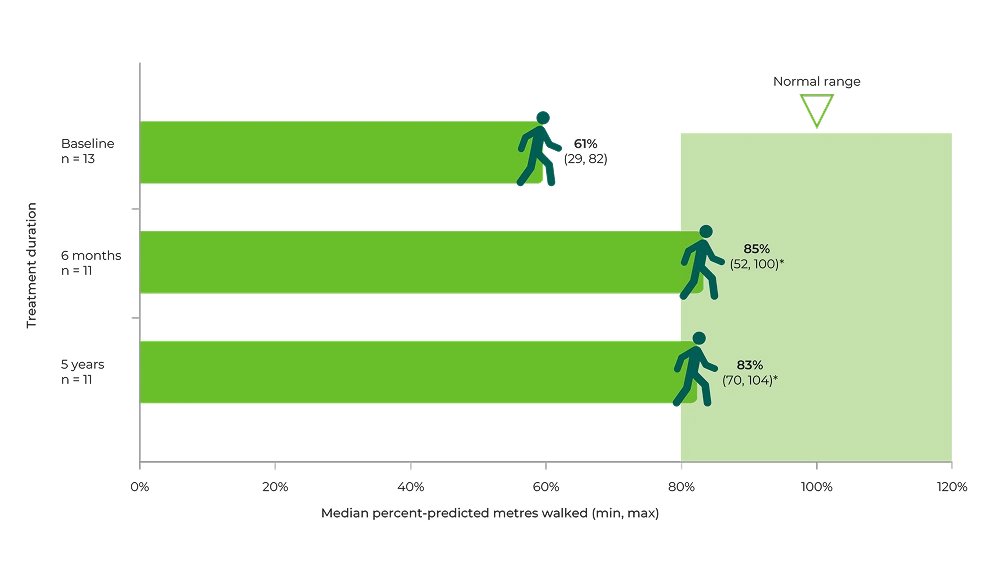
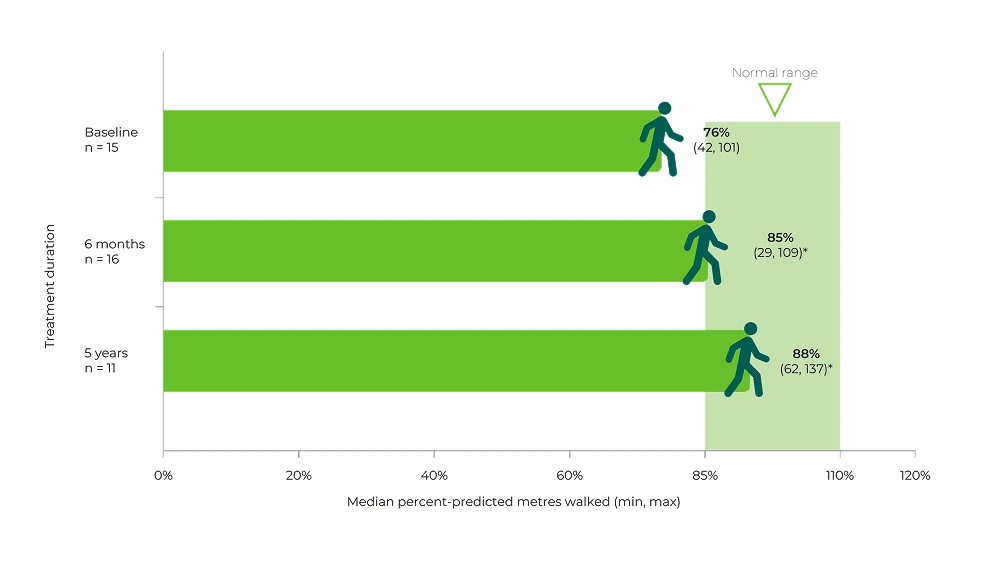
Long-term treatment with STRENSIQ® may help patients with HPP improve the ability to walk independently without the need for assistance6
{kind=link}
The CHAQ discomfort index measures HPP-related pain and is determined by a visual analogue scale of pain (0 = no pain, 100 = very severe pain).12,13
The CHAQ disability index scores range from 0 to 3, with lower scores indicating lower disability. The score is calculated by averaging the highest scores of each of eight domains.12
CHAQ is a validated and sensitive tool for assessing functional status (based on pain and disability) in children with arthritis. It has not been specifically validated in children with HPP.12,13With STRENSIQ®, improvements in pain, disability and strength were observed over 5 years6
- In the STRENSIQ® group, mineralisation lag time decreased significantly by 580% from Baseline to Year 1, indicating improved mineralisation, while changes in osteoid volume and thickness were not statistically significant compared to the control group.8
{kind=link}
STRENSIQ® has demostrated improvements in bone mineralisation lag time and mobility8

▼This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Please report any adverse events via your national reporting system. Adverse events can also be reported to Alexion Pharmaceuticals by the following link: https://contactazmedical.astrazeneca.com/