
ULTOMIRIS® is contraindicated in patients who are not currently vaccinated against Neisseria Meningitidis unless they receive prophylactic treatment with appropriate antibiotics until 2 weeks after vaccination.1 For further information, please visit our dedicated Dosing and Administration and Safety pages.
Please consult the Summary of Product Characteristics prior to prescribing.



*Complete terminal complement inhibition indicated by free C5 in serum <0.5 μg/mL. Sustained terminal complement inhibition throughout the 8-week dosing interval.2,3
¶Complete TMA response, was defined as normalisation of platelet count (≥150 × 109/L), normalisation of serum LDH (≤246 U/L) and ≥25% improvement in serum creatinine from baseline.1
#Among patients with evaluable data, ULTOMIRIS® allowed kidney function recovery (improvement by ≥1 eGFR category stage) vs baseline in 70% (30/43) of adults and 100% (16/16) of paediatric and adolescent patients after 1 year. 17 of the 29 patients who required dialysis at study entry were able to discontinue dialysis by the end of the available follow-up while 6 of 27 patients who were off dialysis at baseline were on dialysis at the end of the initial evaluation period.1 Among patients with aHUS who were on RRT at baseline, ULTOMIRIS® treatment led to dialysis discontinuation in 59% of adults(17/29; median follow-up 76.7 weeks) and 100% of paediatric patients (6/6; follow-up 50 weeks).3,5
¶Complete TMA response, was defined as normalisation of platelet count (≥150 × 109/L), normalisation of serum LDH (≤246 U/L) and ≥25% improvement in serum creatinine from baseline.1
#Among patients with evaluable data, ULTOMIRIS® allowed kidney function recovery (improvement by ≥1 eGFR category stage) vs baseline in 70% (30/43) of adults and 100% (16/16) of paediatric and adolescent patients after 1 year. 17 of the 29 patients who required dialysis at study entry were able to discontinue dialysis by the end of the available follow-up while 6 of 27 patients who were off dialysis at baseline were on dialysis at the end of the initial evaluation period.1 Among patients with aHUS who were on RRT at baseline, ULTOMIRIS® treatment led to dialysis discontinuation in 59% of adults(17/29; median follow-up 76.7 weeks) and 100% of paediatric patients (6/6; follow-up 50 weeks).3,5
aHUS is a form of TMA caused by overactivation of the terminal complement system. aHUS is a life-threatening condition and can lead to stroke, heart attack, kidney failure and premature death6-8. Outcomes for patients with aHUS receiving plasma exchange or plasma infusion (PE/PI) are poor; 45–56% of adults progress to ESRD or die within 1 year9,10, and up to 77% have ESRD or die within 3 years.11
Rapid identification of TMA, diagnosis of aHUS and urgent initiation of targeted treatment are crucial in preserving renal function and improving outcomes.6,12
Rapid identification of TMA, diagnosis of aHUS and urgent initiation of targeted treatment are crucial in preserving renal function and improving outcomes.6,12
{kind=link}
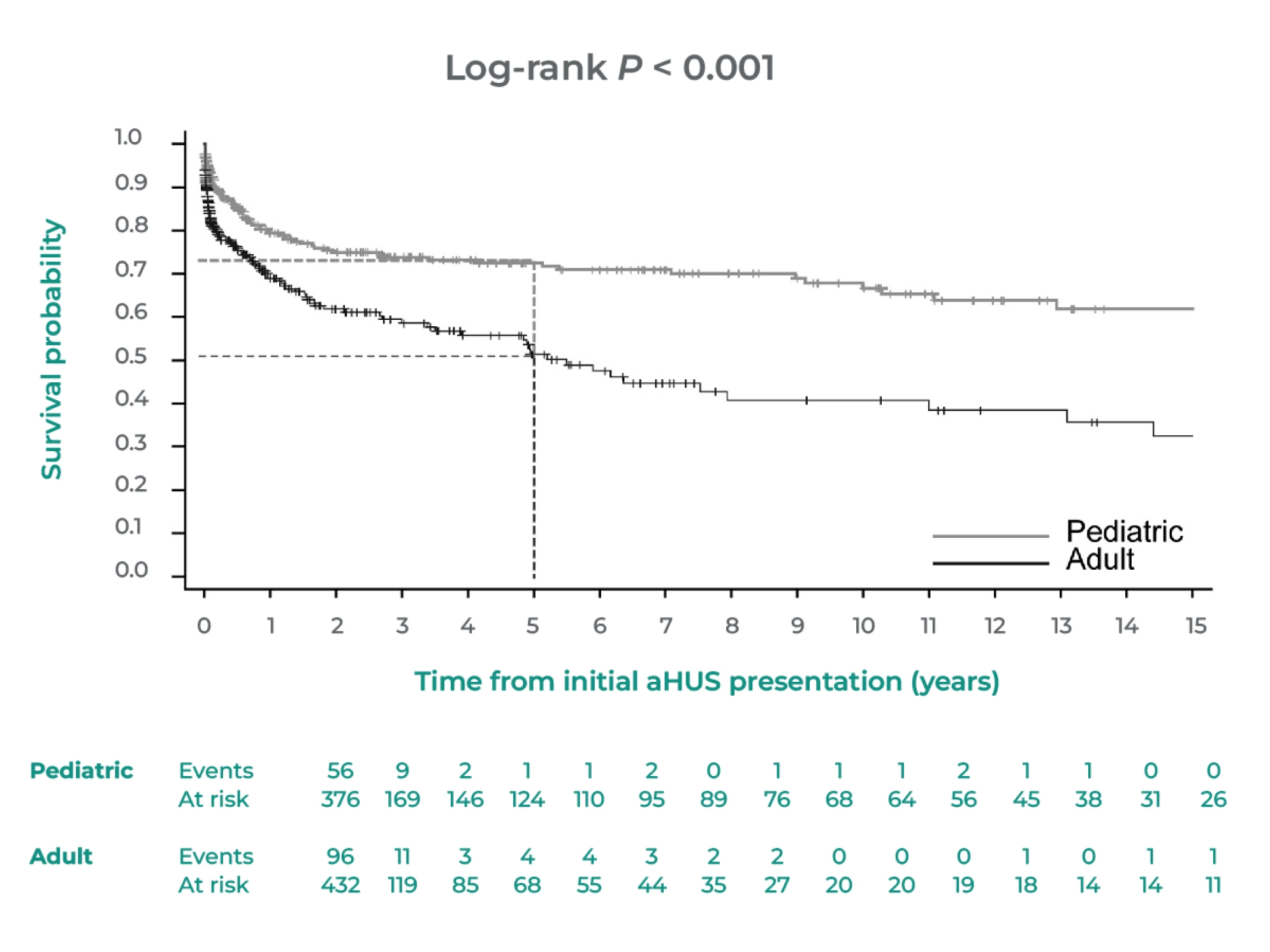
Graph adapted from Schaefer, Franz et al. 2018.13
Cumulative Kaplan-Meier estimates for end-stage renal disease survival probability analyzed according to adult and pediatric age at initial presentation
Number of patients at risk shown for every year after initial atypical hemolytic uremic syndrome (aHUS ) presentation.
End-stage renal disease analysis excludes those patients with kidney transplant prior to aHUS presentation ( n = 36 ) and those with eculizumab initiation at aHUS presentation ( n =7 ).13
Cumulative Kaplan-Meier estimates for end-stage renal disease survival probability analyzed according to adult and pediatric age at initial presentation
Number of patients at risk shown for every year after initial atypical hemolytic uremic syndrome (aHUS ) presentation.
End-stage renal disease analysis excludes those patients with kidney transplant prior to aHUS presentation ( n = 36 ) and those with eculizumab initiation at aHUS presentation ( n =7 ).13
ESRD or Death
46% (57/125)
46% (57/125)
ESRD or Death
71% (89/125)
71% (89/125)
ESRD or Death
17% (15/89)
17% (15/89)
ESRD or Death
39% (35/89)
39% (35/89)
§Retrospective analysis of 125 adult (≥ 16 years) and 89 paediatric French patients with aHUS assessed the effect of complement gene mutations on disease onset, presentation, and outcome.9
†Median follow-up of 57 months (range, 1-353 months).9
‡Median follow-up of 45 months (range, 1-493 months).9
†Median follow-up of 57 months (range, 1-353 months).9
‡Median follow-up of 45 months (range, 1-493 months).9

Adverse Event Reporting
Please report any adverse events via your national reporting system. Adverse events can also be reported to Alexion Pharmaceuticals by contacting: https://contactazmedical.astrazeneca.com/
C5, complement component 5; aHUS, Atypical haemolytic uraemic syndrome; ESRD, end-stage renal disease; LDH, lactate dehydrogenase; PE, plasma exchange; PI, plasma infusion; RRT, renal replacement therapy; TMA, thrombotic microangiopathy.