
The National Cancer Institute (NCI) natural history study followed 41 patients with NF1 for 7 years, assessing PN volume and PN-related morbidities in 57 distinct PN.3 Of these, 49 (86%) PN had a > 20% increase in volume from baseline to maximum assessment.3 The median PN volume change from baseline to maximum assessment was 108.9% (range: -2.15% to 790%), with a median growth rate of 15.9% (lower quartile: 10.1%; upper quartile: 28.0%).3 The study showed that NF1-PN grow most rapidly in patients aged 3–5 years, with a median growth rate of 35.1% per year compared with 13.1% in patients aged 11–25 years.3
These findings are consistent with previous longitudinal studies in Germany and the US, where NF1-PN growth rate was observed to be inversely related to age, and fastest in patients aged <21 years.4,5
These findings are consistent with previous longitudinal studies in Germany and the US, where NF1-PN growth rate was observed to be inversely related to age, and fastest in patients aged <21 years.4,5




Most patients with NF1-PN (n = 36/41) in the NCI natural history study had PN that caused morbidity at the time of first assessment.3 In all patients with morbidity caused by PN at the time of first assessment, morbidity was still present after ≥ 7 years of follow-up.3
{kind=link}
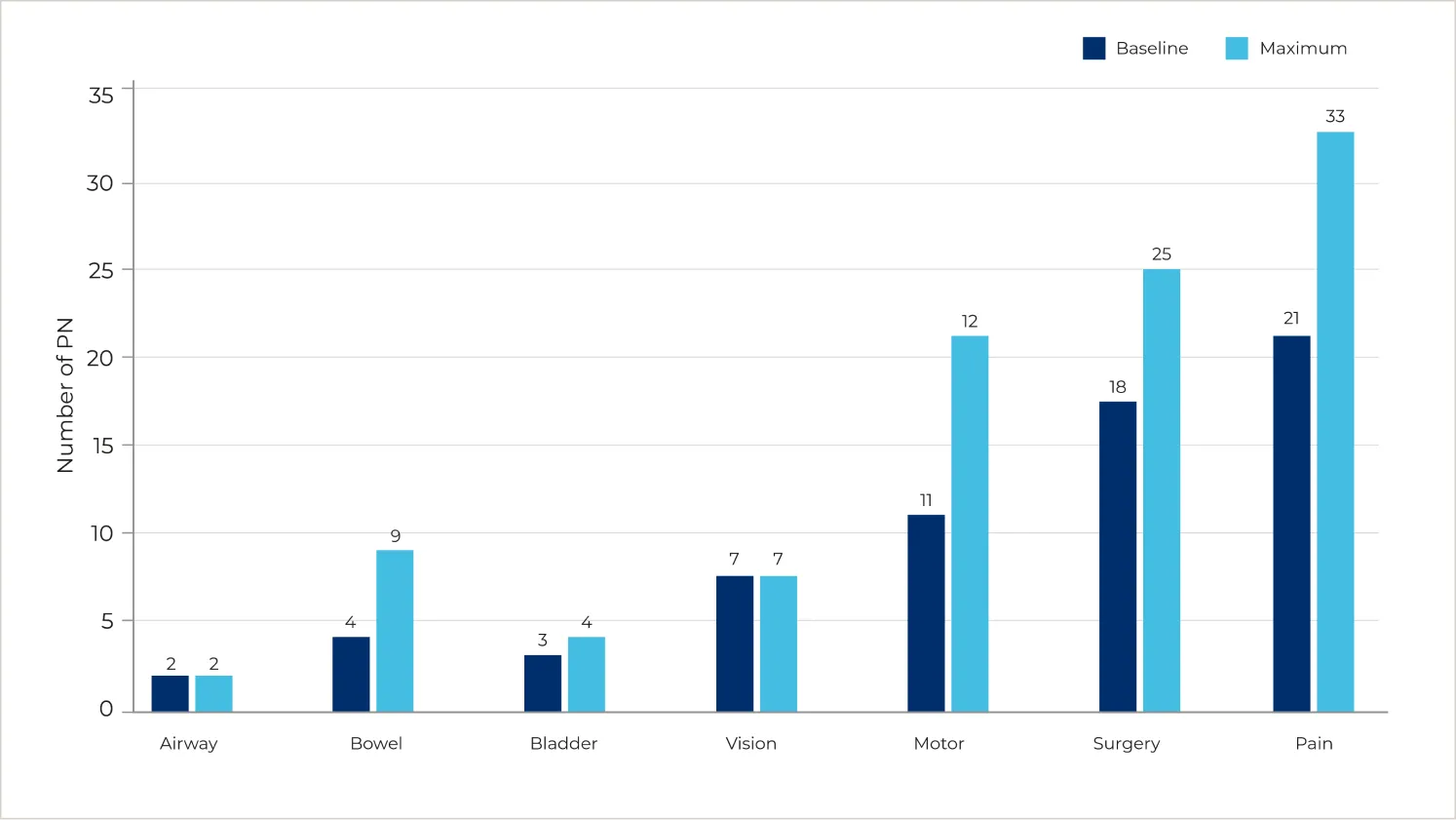
Adapted from: Gross AM et al. Neuro Oncol. 2018;20(12):1643–1651.3
An analysis of patients with NF1-PN with ≥ 7 years of follow-up data available (N = 41, median age at enrolment 13 years) showed that PN-related morbidities became more frequent over time, and almost never resolved or improved spontaneously.3
An analysis of patients with NF1-PN with ≥ 7 years of follow-up data available (N = 41, median age at enrolment 13 years) showed that PN-related morbidities became more frequent over time, and almost never resolved or improved spontaneously.3
PN-related morbidities are primarily caused by their impact on surrounding structures and the severity of complications generally increases with tumour volume.7 These morbidities can be life-threatening; based on a retrospective review of 154 patients with NF1-PN seen at Cincinnati Children Hospital Medical Center between 1997 and 2007, patients with symptomatic PN have a higher mortality rate (3.2%) compared to patients with NF1 with asymptomatic PN or without PN.7,8
A study of 140 children aged between 8–17 years with NF1-PN (symptomatic or asymptomatic PN) recruited from the Children’s Tumour Foundation NF Patient Registry, US NF1 organisations and the Children’s Hospital of Chicago completed two quality of life questionnaires (Patient-Reported Outcomes Measurement Information System [PROMIS] and the Quality of Life in Neurological Disorders [Neuro-QoLTM) via computerised adaptive tests.9 Respondents reported worse scores compared with US norms on 8 of 10 domains, which included anxiety, depression, mobility and peer relationships.9
Adapted from: Lai JS et al. J Pediatr. 2019;206:190–196.9
Scores were reported using a T-score metric with a norm of 50 and standard deviation of 10.
Study limitations included that scoring was reported by parents without access to medical records and socioeconomic status and other environmental factors were not taken into account.9
A: Scores > 50 represent worse functioning compared to the US general population. The standard deviation was wider than the norm in all domains except for stigma and psychological stress response.9
B: Scores < 50 represent worse functioning compared to the US general population. Except for upper extremity functioning, the standard deviation of the other measures was below the norm.9
Scores were reported using a T-score metric with a norm of 50 and standard deviation of 10.
Study limitations included that scoring was reported by parents without access to medical records and socioeconomic status and other environmental factors were not taken into account.9
A: Scores > 50 represent worse functioning compared to the US general population. The standard deviation was wider than the norm in all domains except for stigma and psychological stress response.9
B: Scores < 50 represent worse functioning compared to the US general population. Except for upper extremity functioning, the standard deviation of the other measures was below the norm.9
Social and emotional functioning can also be affected in those with NF1-PN. A US-based cross-sectional study of the parents and teachers of 53 children aged 6–18 years (mean age: 12.4 ± 3.4 years) found a notable proportion of the children had clinically significant or at-risk scores on subscales of the Behaviour Assessment System for Children–Second Edition (BASC-2), including somatisation (42%), attention problems (32%), and depression (30%).10
Patient reported outcomes, including QoL, in paediatric patients with NF1 is an active area of research. Limitations of published studies include a lack of validated instruments in NF1, small sample size, and valid comparators, especially for children younger than 8.11,12 The Response Evaluation in Neurofibromatosis and Schwannomatosis (REiNS) International Collaboration is in the process of evaluating existing self- and parent-reported measures for NF1, rating the Pediatric Quality of Life Inventory (PedsQL) highest for use in both medical and psychosocial trials of paediatric patients with NF1.11
Patient reported outcomes, including QoL, in paediatric patients with NF1 is an active area of research. Limitations of published studies include a lack of validated instruments in NF1, small sample size, and valid comparators, especially for children younger than 8.11,12 The Response Evaluation in Neurofibromatosis and Schwannomatosis (REiNS) International Collaboration is in the process of evaluating existing self- and parent-reported measures for NF1, rating the Pediatric Quality of Life Inventory (PedsQL) highest for use in both medical and psychosocial trials of paediatric patients with NF1.11
Caregiver burden
The burden among carers of paediatric patients with NF1-PN is also substantial. A US-based study surveyed 95 carers of paediatric patients with NF1 aged 2–18 years in the US in which 14% and 11% of carers were diagnosed with NF1 and NF1-PN respectively.13 The study found that 53% (n = 50/95) of carers reported at least mild-to-moderate burden using the Zarit Burden Interview.13 Additionally, 48% (n = 46/95) reported having anxiety, and 35% (n = 33/95) were found to have depression.13
As well as psychological impacts, employed carers (N = 56) also reported a reduced ability to attend work, with a mean 2.4 (standard deviation: 5.1) hours of work missed in the past week and an average loss of 22.3% (standard deviation: 25.0%) in productivity at work (presenteeism and absenteeism) in the past week.13
Among the whole sample (N = 95), an average of 17.2% (standard deviation: 22.5%) of activities of daily living other than work were impaired as a result of caring for a patient with NF1-PN.13
As well as psychological impacts, employed carers (N = 56) also reported a reduced ability to attend work, with a mean 2.4 (standard deviation: 5.1) hours of work missed in the past week and an average loss of 22.3% (standard deviation: 25.0%) in productivity at work (presenteeism and absenteeism) in the past week.13
Among the whole sample (N = 95), an average of 17.2% (standard deviation: 22.5%) of activities of daily living other than work were impaired as a result of caring for a patient with NF1-PN.13
BASC-2, Behaviour Assessment System for Children–Second Edition; NCI, National Cancer Institute; NF1, neurofibromatosis type 1; PedsQL, Pediatric Quality of Life Inventory; PN, plexiform neurofibroma; PROMIS, Patient-Reported Outcomes Measurement Information System; Neuro-QoL, Quality of Life in Neurological Disorders; QoL, quality of life; REiNS, Response Evaluation in Neurofibromatosis and Schwannomatosis..
healthcare professional