
healthcare professional
The primary endpoint of CHAMPION-NMOSD was time to first adjudicated on-trial relapse and associated relapse risk reduction in the ravulizumab group compared with the placebo group.2
No adjudicated relapse occurred during 84 patient-years of treatment with ULTOMIRIS® (n = 58) vs placebo (n = 47) (from the PREVENT study) during 46.9 patient years (P < 0.001).2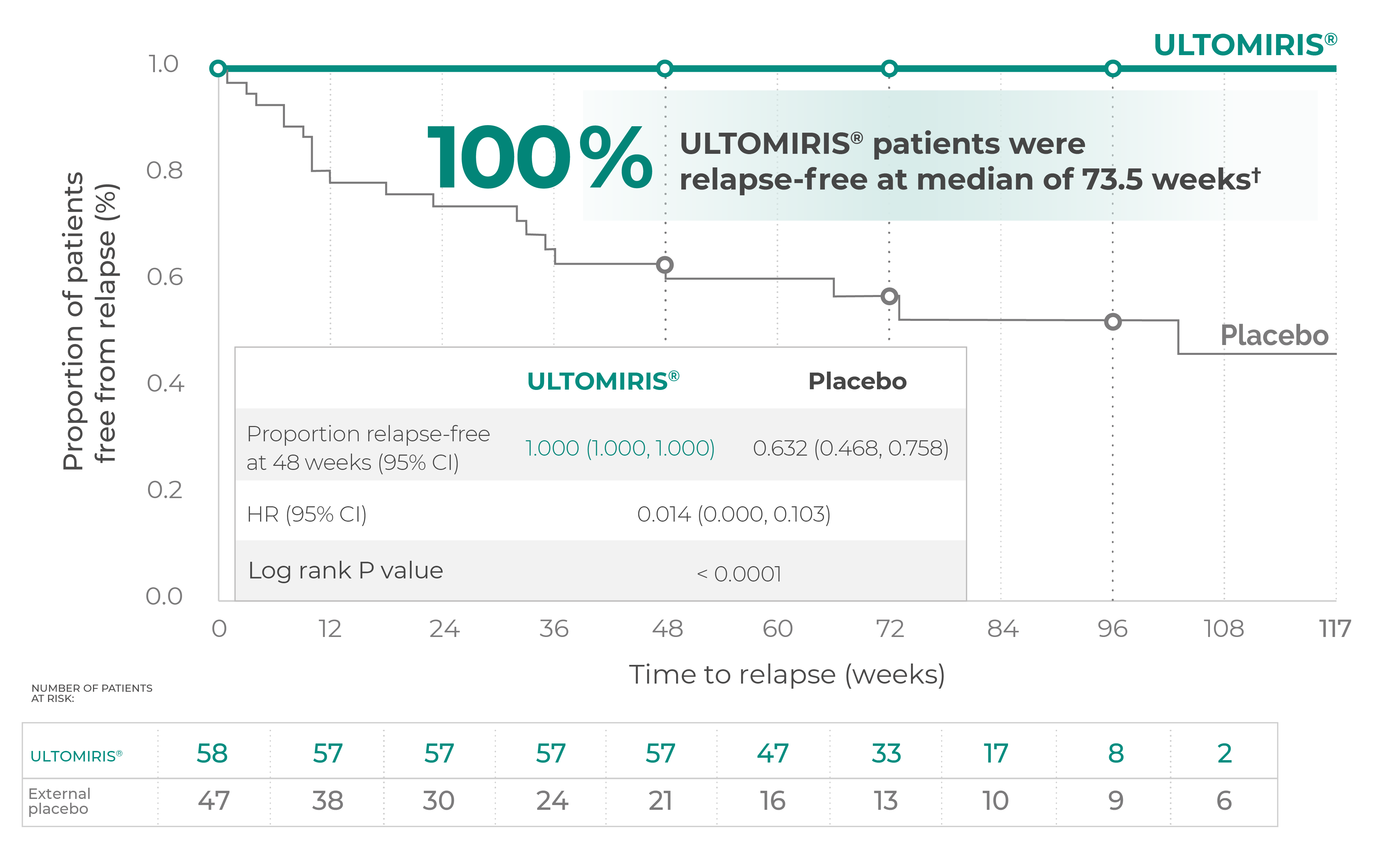{kind=link}
Adapted from Pittock SJ, et al. Ann Neurol. 2023;93(6):1053–1068.
* Patients were allowed to have concomitant IST treatment.2
† Range (11.0–117.7 weeks).2
Limitations regarding the use of an external control to estimate the treatment effect should be considered when interpreting these data.2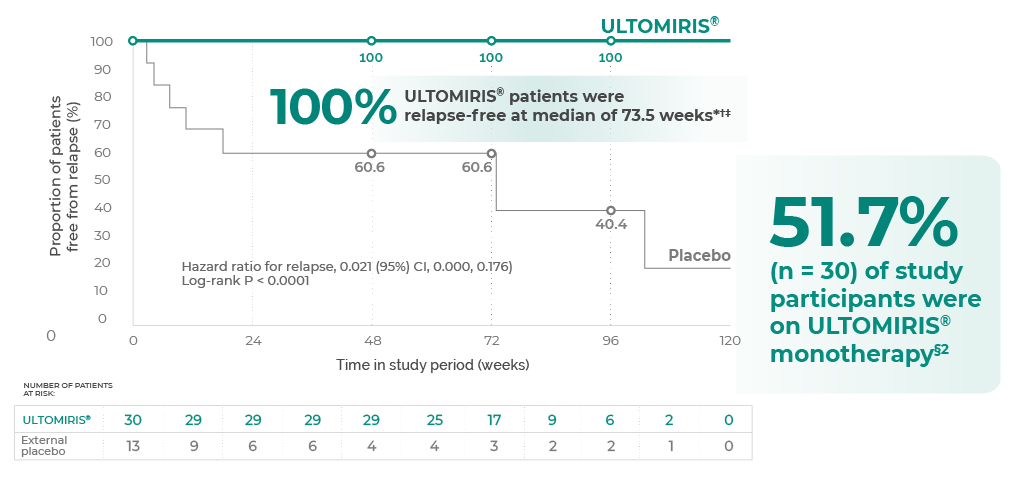{kind=link}
* P < 0.0001; HR = 0.021 (95% CI: 0.000, 0.176).2
† Patients who did not receive ISTs at baseline.2
‡ Range (11.0–117.7 weeks).2
§ 27.7% (n = 13) of study participants receiving placebo didn't receive IST at baseline.2
Limitations regarding the use of an external control to estimate the treatment effect should be considered when interpreting these data.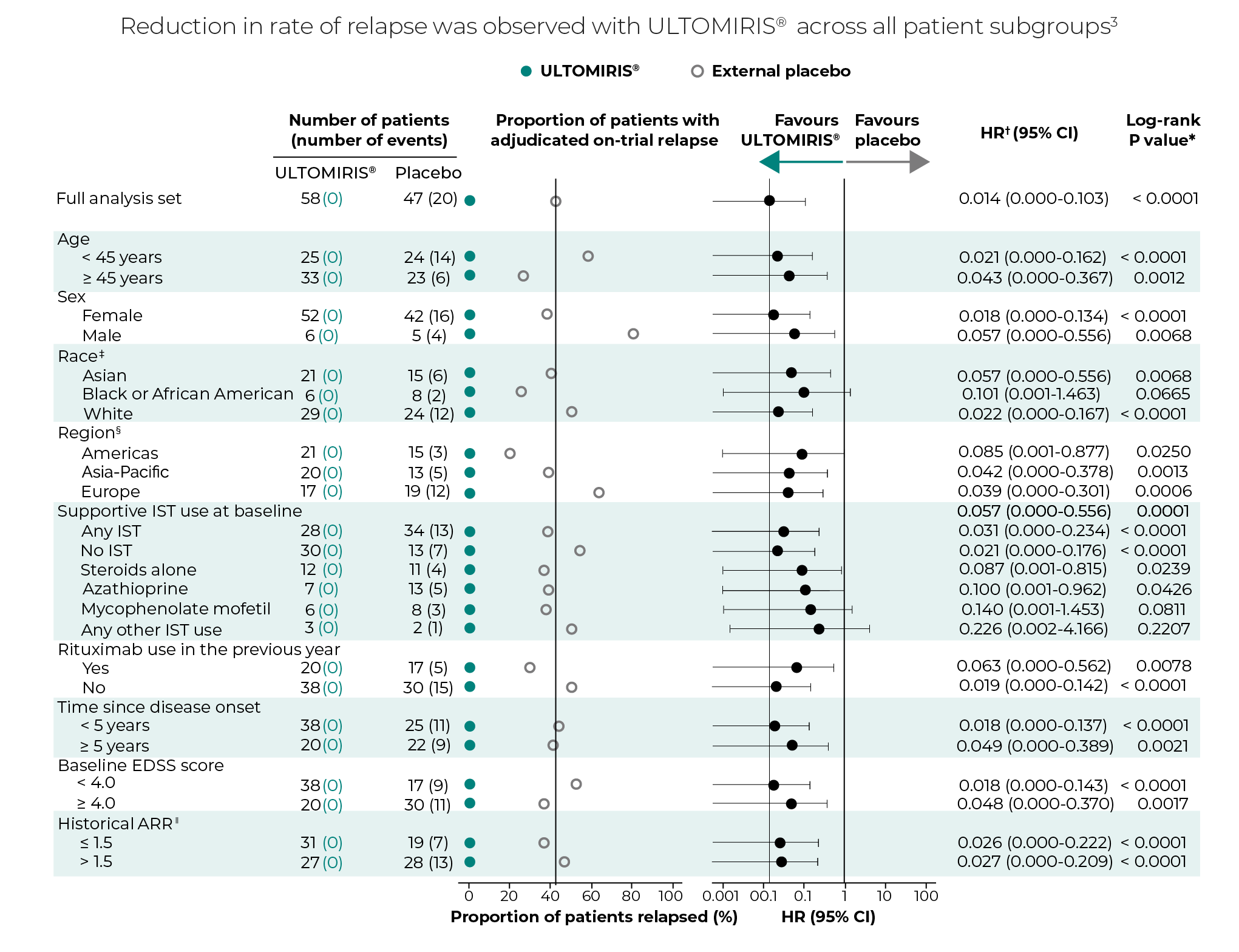{kind=link}
Adapted from Pittock SJ, et al. CHAMPION-NMOSD Subgroup analysis poster.
* Not all comparisons were statistically significant.3
† Based on a Cox proportional hazards model with treatment covariate. Firth’s adjustment with profile likelihood confidence limits applied.3
‡ Unknown race excluded from forest plot.3
§ Americas: Argentina, Canada and the USA; Europe: Croatia, Denmark, Germany, Italy, Poland, Russia, Spain, Turkey and the UK; Asia-Pacific: Australia, Hong Kong, Japan, the Republic of Korea and Taiwan.3
‖ Within the previous 24 months.3
{kind=link}
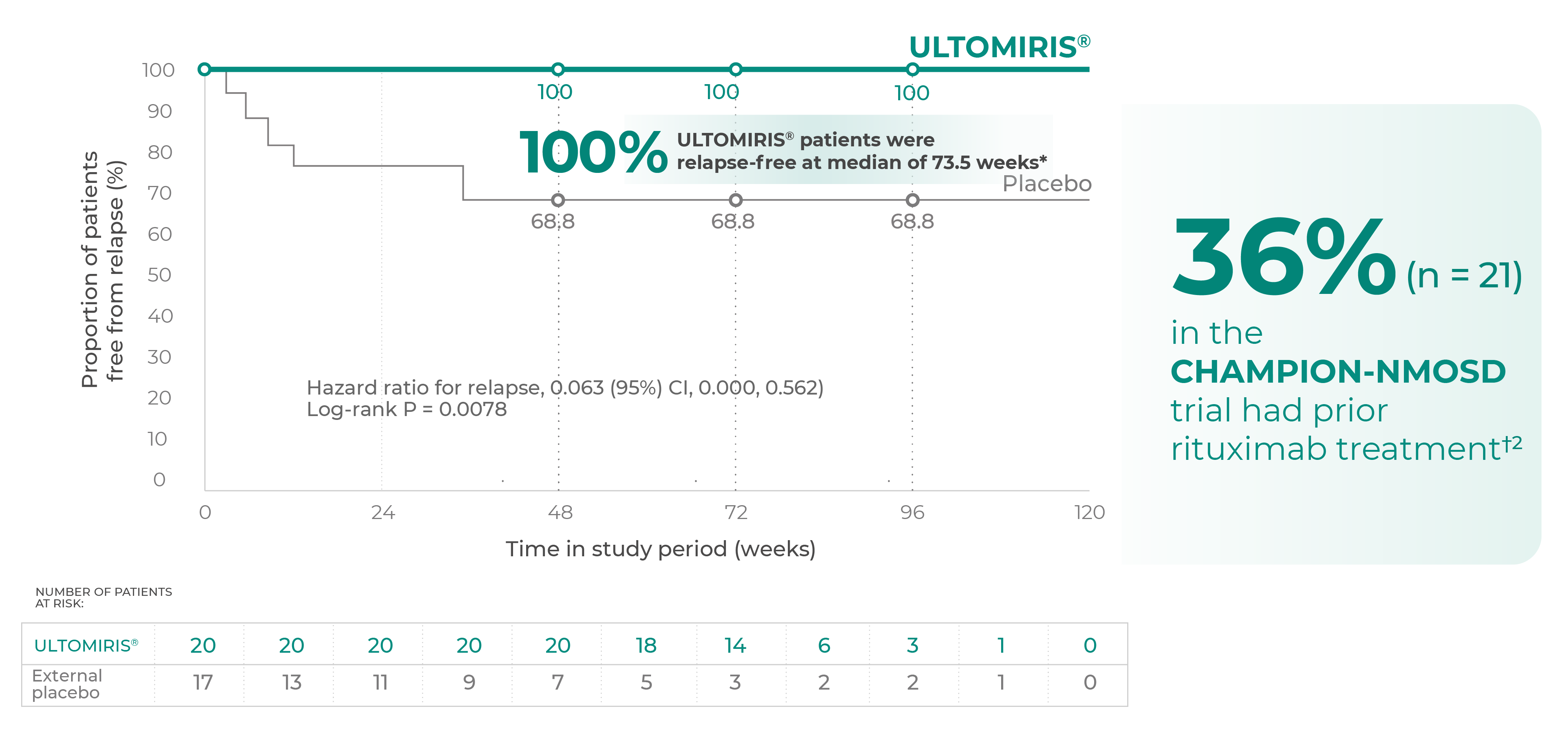
* In the 12 months before screening.2
† Rituximab was not permitted as a concomitant IST in CHAMPION-NMOSD. Patients who received rituximab during the 3 months before screening were excluded from the trial.2- HAI is a rating scale, used to assess mobility, by evaluating the time and degree of assistance required to walk 25 feet
- Even after their first attack, patients may develop disabilities that rank anywhere on the HAI; as a result, subsequent attacks may be even more debilitating

Adapted from Pittock SJ, et al. Ann Neurol. 2023;93(6):1053–1068.
* Vs external placebo, other secondary endpoints were not statistically significant.2
† The ARRRav was tested against a null hypothesis of 0.25. The comparator rate of 0.25 was chosen to represent a conservative ARR that may be experienced in the NMOSD patient population.2
‡ Per the statistical analysis plan, no relapses would be statistically significant. Because the Poisson regression would not run with 0 relapses the P value and upper CI are from an ad hoc exact test.2
§ HAI scores range from 0 to 9, with higher scores indicating decreased independent ambulation.2
‖ Clinically important worsening in HAI score was conditional on the baseline value and was defined as a baseline HAI score of 0 with a subsequent increase of ≥2 points or a baseline HAI score > 0 with a subsequent increase of ≥ 1 point. The analysis was performed using logistic regression, adjusting for baseline HAI.2
¶ EQ-5D index scores range from 0 (with 0 being the value of a health state equivalent to dead) to 1 (the value of full health), with higher scores indicating higher health utility. The analysis was performed using ranked analysis of covariance, adjusting for the baseline value.2
# EQ-5D VAS scores range from 0 (the worst imaginable health) to 100 (the best imaginable health), with higher scores indicating higher perceived quality of health. The analysis was performed using analysis of covariance of the ranks of the change from baseline, adjusting for the ranks of the baseline values.2
Δ Because statistical significance for clinically important change from baseline in EQ-5D score was not met, P values for subsequent lower-ranking secondary efficacy endpoints are not presented.2
◊ EDSS scores ranged from 0 (no disability) to 10 (death).2
↓ Clinically important worsening in EDSS score was conditional on the baseline value and was defined as a baseline EDSS score of 0 with a subsequent increase of ≥ 2 points, a baseline EDSS score between 1 and 5 with a subsequent increase of ≥ 1 point, or a baseline EDSS score > 5 with a subsequent increase of ≥ 0.5 points. The analysis was performed using logistic regression, adjusting for baseline EDSS.2
During the trial, there were 2 non-adjudicated relapses which were intervened with PP and IVIg.9
CHAMPION-NMOSD study limitation: physician-reported endpoints were part of an exploratory analysis and should be considered for contextualization only. Results or clinical outcomes should be interpreted with caution.
The rates of annualized On-trial relapse-related (as determined by the Treating Physician) hospitalizations and acute
treatments were collected as additional study endpoints, and were not primary endpoints.8
Adverse Event Reporting
Please report any adverse reactions via your national reporting system. Adverse events should also be reported to Alexion pharmaceuticals by the following link: https://contactazmedical.astrazeneca.com