
▼This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Please report any adverse events via your national reporting system. Adverse events can also be reported to Alexion Pharmaceuticals by contacting: https://contactazmedical.astrazeneca.com.
Please refer to the Summary of Product Characteristics for further information.
healthcare professional




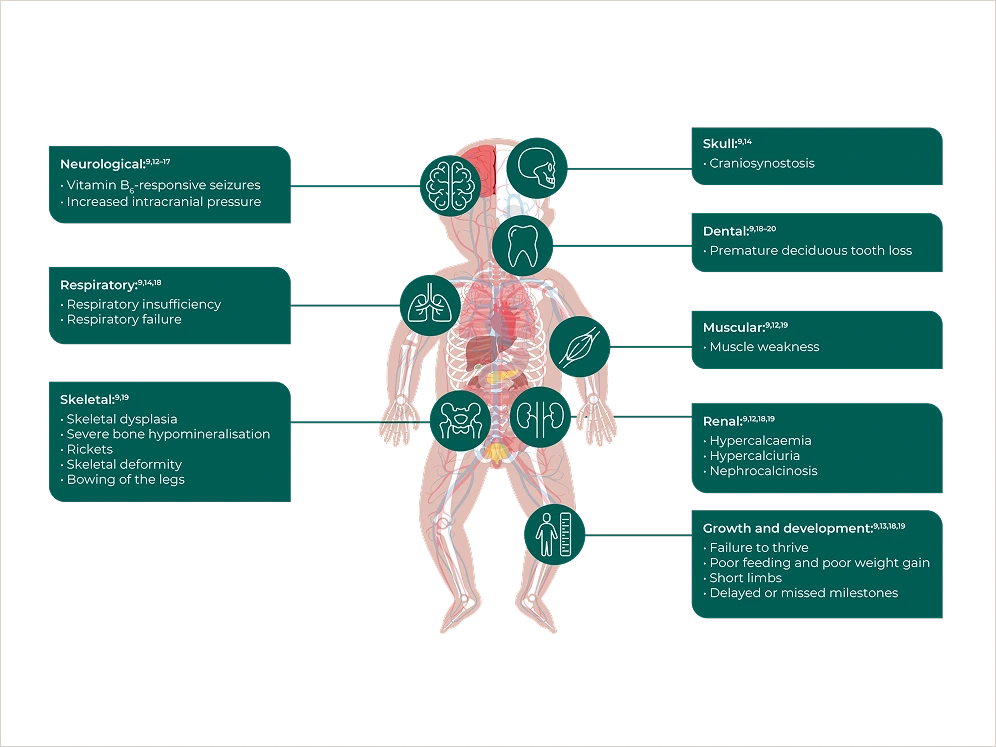
HPP is characterised by persistently low ALP activity, impaired bone mineralisation, muscle weakness and other systemic manifestations.8–10
- HPP is caused by deficient activity of an enzyme, TNSALP, which is encoded by the ALPL gene8–11*
* Different isoforms of ALP exist; however the majority is TNSALP.11,12
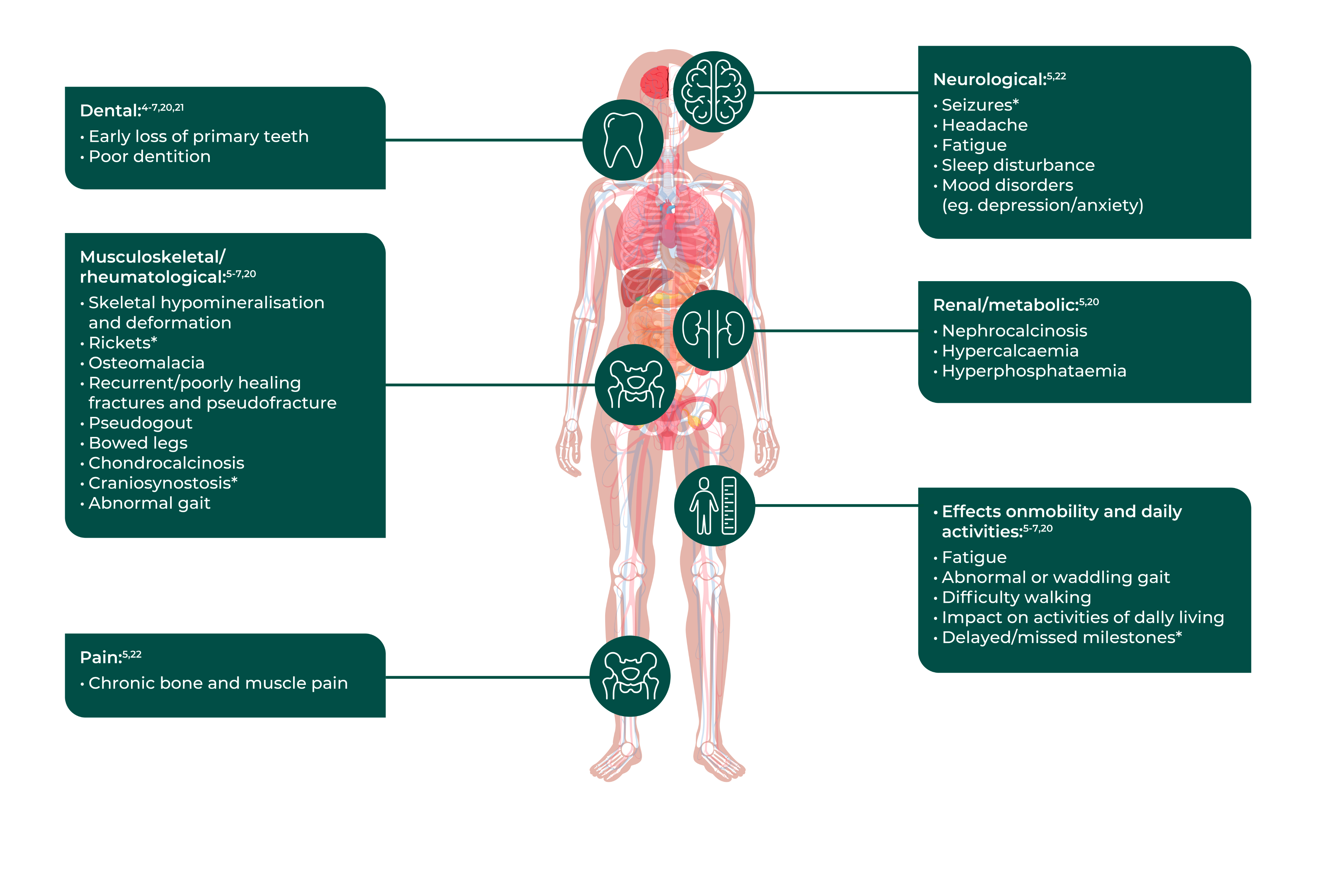
The clinical presentation of HPP can differ in its signs and symptoms.8–10
{kind=link}
{kind=link}
Mortality is high in perinatal and infantile-onset populations, primarily as a result of respiratory failure and/or other complications due to impaired bone mineralisation and chest deformity.19,22
Pain, dental problems†, skeletal, constitutional/metabolic, and muscular manifestations were most frequently reported

67.3% (n/N=202/300) of adult patients reported pain, 30.2%‡ (n/N=79/262) received medication for pain, 11.8%‡ (n/N=31/262) reported taking opioids

62.1%‡ (n/N=149/240) had a history of ≥ 1 fracture/pseudo-fracture and 37.8%‡ (n/N=102/270) of patients experienced ≥ 5 HPP manifestations, highlighting that HPP is a systemic disease with wide-ranging effects
Surgical intervention was required for 28.2%‡ (n/N=42/149) of those patients who had ≥ 1 fracture/pseudo-fracture before treatment, and 54.3%‡ (n/N=163/300) reported early loss of deciduous teeth, loss of permanent teeth and poor dentition

Of those who reported to use ≥ 1 assistive device for disability or home modification, assistive devices in use were crutches (39.0%‡) and a cane (34.1%‡); home modifications were widely reported

* As seen in the Global HPP Registry, an observational, longitudinal, multinational long-term study collecting data on HPP diagnosis, history, clinical course, symptoms (including multisystemic aspects of disease) and burden of illness from patients who have a diagnosis of HPP. 304 adults with a confirmed diagnosis of HPP who met the analysis criteria were included within this analysis.24
† Including early loss of deciduous teeth, loss of permanent teeth and poor dentition.24
‡ Of those with available data.24
ALP, alkaline phosphatase; HPP, hypophosphatasia; TNSALP, tissue non-specific alkaline phosphatase.
This medicinal product has been authorised under ‘exceptional circumstances’. This means that due to the rarity of the disease it has not been possible to obtain complete information on this medicinal product.
▼This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Please report any adverse events via your national reporting system. Adverse events can also be reported to Alexion Pharmaceuticals by the following link: https://contactazmedical.astrazeneca.com/
▼This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Please report any adverse events via your national reporting system. Adverse events can also be reported to Alexion Pharmaceuticals by the following link: https://contactazmedical.astrazeneca.com/