
The endothelial cells are then damaged or destroyed leading to a TMA, with clotting in the small vessels and ischemic damage to the downstream organs.6
Often there is a precipitating infection, illness, or event (e.g., surgery or pregnancy) that activates the alternate complement pathway, but then this system fails to turn itself off.6,7
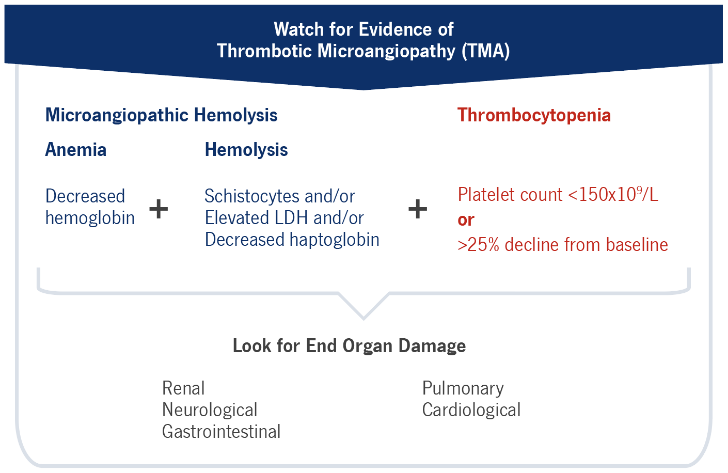
Every organ in the body can be damaged.8The brain and kidneys are most often affected, with loss of kidney function a common result. Mortality in the first episode is 10–15%, rising when diagnosis and treatment is delayed.
{kind=link}
A.K.A. Complement-mediated Hemolytic Uremic Syndrome (CM-HUS)
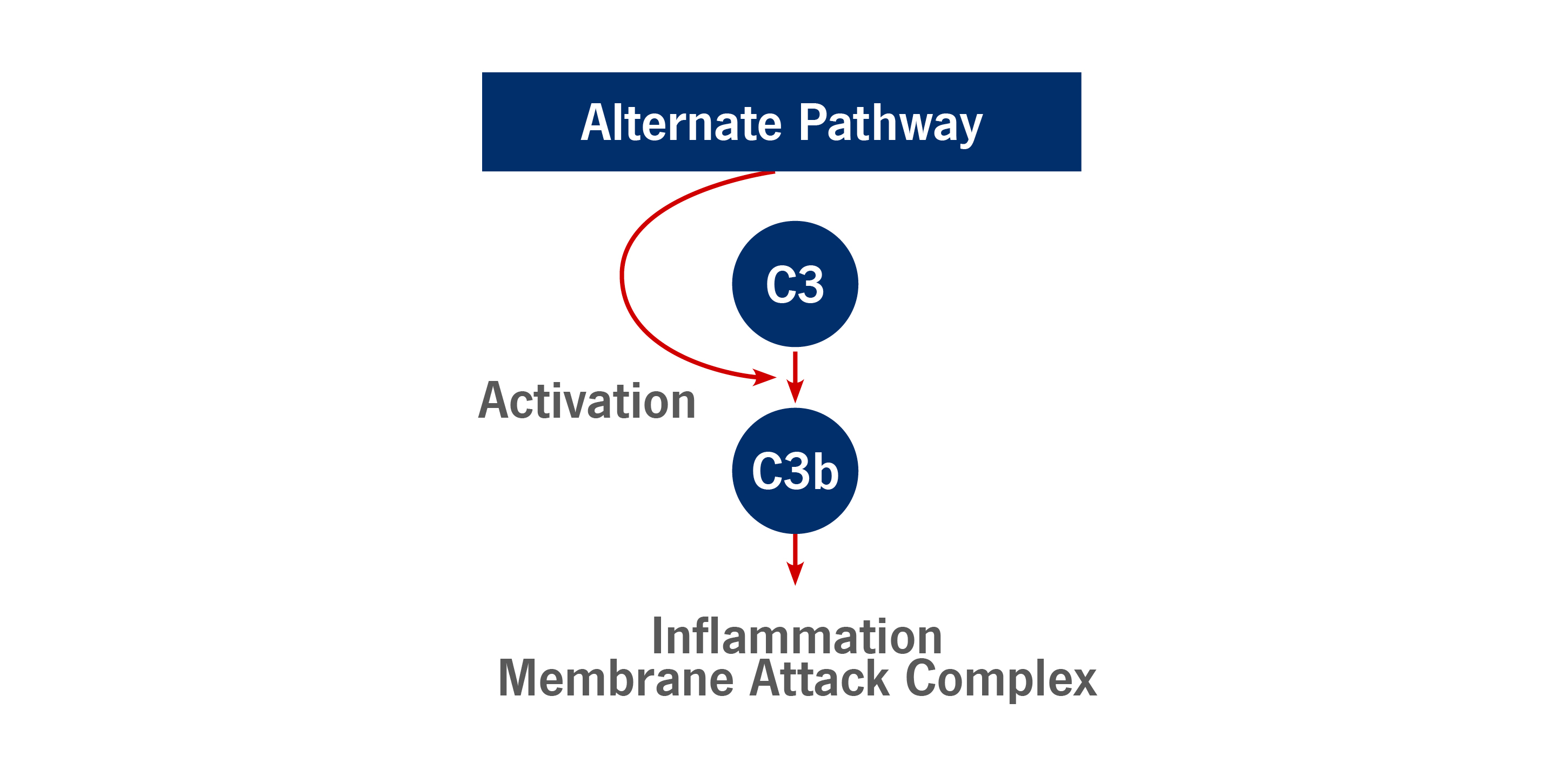
Inappropriate activation of the alternate complement pathway- Gain of function mutations in promoters
- Loss of function mutations in inhibitors
- Inhibitor antibody
- Up to 30% don’t have a known mutation or antibody9
{kind=link}

{kind=link}
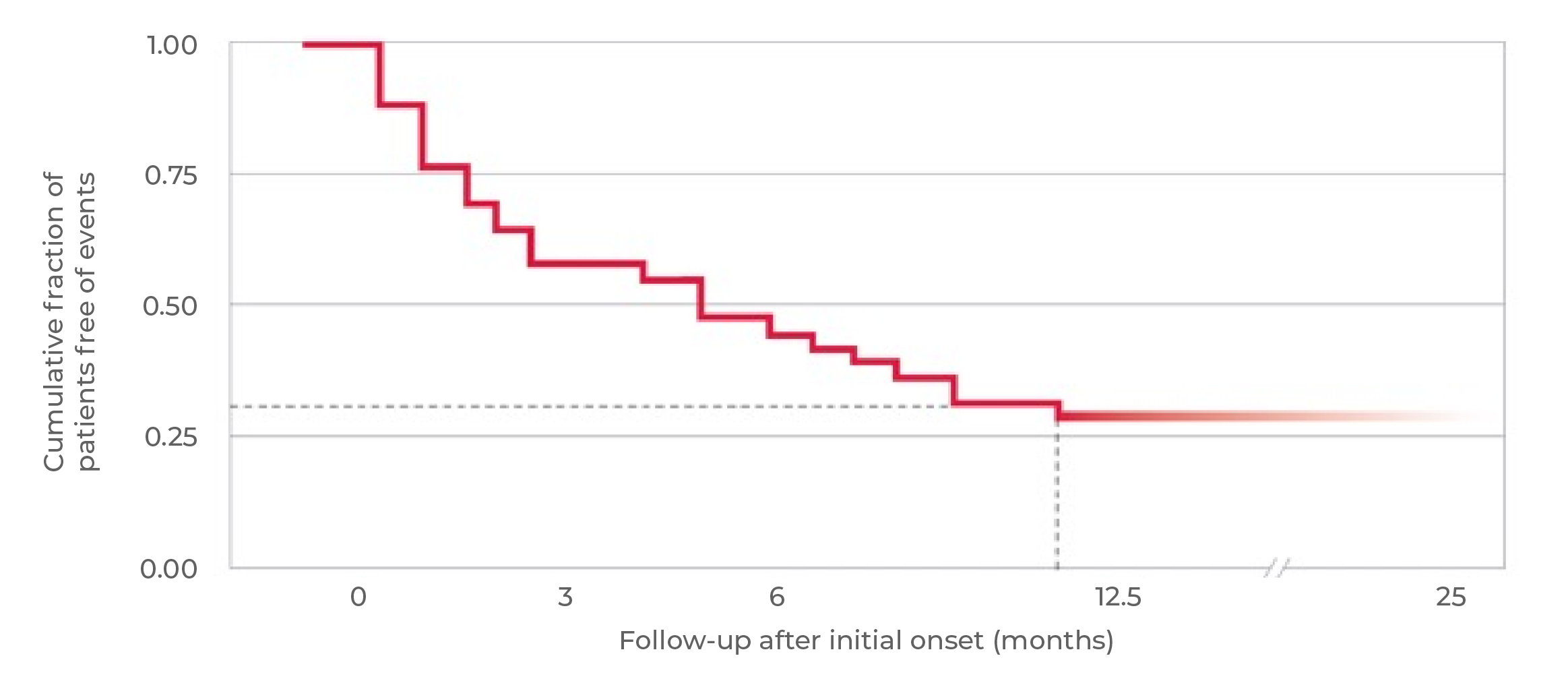
of all patients progress to end-stage renal disease (ESRD) or die with the first clinical manifestation11
of all patients have permanent renal damage, require dialysis, or die within 3 years9
Study description: An analysis of the outcomes in 40 patients with the complement factor H (CFH) mutation.
The cumulative fraction of patients free of events was estimated by Kaplan–Meier analysis.11
{kind=link}
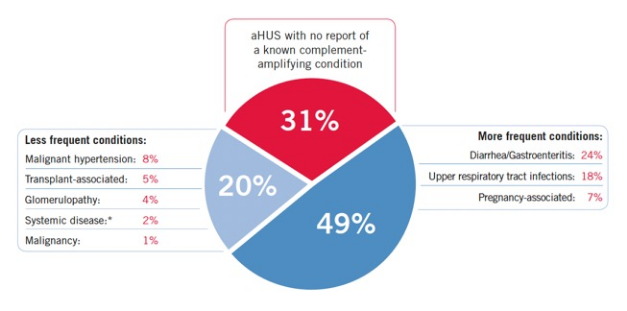
Study description: Analysis of 191 patients with aHUS and data available for reports of triggering/underlying conditions, registered consecutively from 1996 to 2007 within the International Registry of Recurrent and Familial HUS/TTP.9
*E.g., systemic lupus erythematosus and scleroderma.
Persistent TMA, however, is uncommon in these complementamplifying conditions once adequately treated.12
{kind=link}
Indications and Clinical Use:
ULTOMIRIS® (ravulizumab for injection) is indicated for:
- The treatment of adult and pediatric patients one month of age and older with atypical hemolytic uremic syndrome (aHUS) to inhibit complement-mediated thrombotic hemolysis (TMA)
Limitations of Use: ULTOMIRIS® is not indicated for the treatment of patients with Shiga toxin E. coli related hemolytic uremic syndrome (STEC-HUS).
Contraindications:- Do not initiate ULTOMIRIS® in patients with unresolved Neisseria meningitidis infection
Most Serious Warnings and Precautions:
- Comply with the most current National Advisory Committee on Immunization (NACI) recommendations for meningococcal vaccination in patients with complement deficiencies.
- Patients must be vaccinated against meningococcal infections prior to, or at the time of, initiating ULTOMIRIS®, unless the risks of delaying ULTOMIRIS® therapy outweigh the risks of developing a meningococcal infection.
- Monitor patients for early signs of meningococcal infections and treat immediately if infection is suspected.
Please consult the product monograph https://alexion.com/documents/ultomiris_product_monograph_approved_english for important information relating to adverse reactions, drug interactions, and dosing information which have not been discussed in this piece. The product monograph is also available by calling 1-844-922-0605.
Indications and Clinical Use:
SOLIRIS® (eculizumab for injection) is indicated for:
- The treatment of patients with atypical hemolytic uremic syndrome (aHUS) to reduce complement-mediated thrombotic microangiopathy.
Contraindications:
Do not initiate SOLIRIS® in patients:
- with unresolved Neisseria meningitidis infection
- who are not currently vaccinated against Neisseria meningitidis (unless they receive prophylactic treatment with appropriate antibiotics until 2 weeks after vaccination)
Most Serious Warnings and Precautions:
- Comply with the most current National Advisory Committee on Immunization (NACI) recommendations for meningococcal vaccination in patients with complement deficiencies.
- All patients must be vaccinated with meningococcal vaccines prior to, or at the time of, initiating SOLIRIS®, unless the risks of delaying SOLIRIS® therapy outweigh the risks of developing a meningococcal infection; revaccinate according to current medical guidelines for vaccine use.
- All patients must be monitored for early signs of meningococcal infections, evaluated immediately if infection is suspected, and treated with antibiotics, if necessary.
Please consult the product monograph https://alexion.com/-/media/alexion_global/documents/regulatory/north-america/canada/2024/english/soliris_product_monograph_en_approved_24jul2024.pdf for important information relating to adverse reactions, drug interactions, and dosing information which have not been discussed in this piece. The product monograph is also available by calling 1-844-922-0605.